When it comes to gait, getting the 1st ray to the ground is the name of the game. When weight travels through the medial forefoot and we are able to push off the 1st ray complex, that is called "high gear push off". This was 1st discussed F Bojsen-Møller in this excellent paper (1), that just happens to be a free full text! Craig Payne, The Running Research Junkie has offered and excellent commentary on the topic here as well.
High Gear Push Off can happen when 3 conditions are met:
- we have a intact visual, vestibular and kinesthetic systems that ensure we can remain upright in the gravitational plane.
- we have an intact calcanocuboid locking mechanism
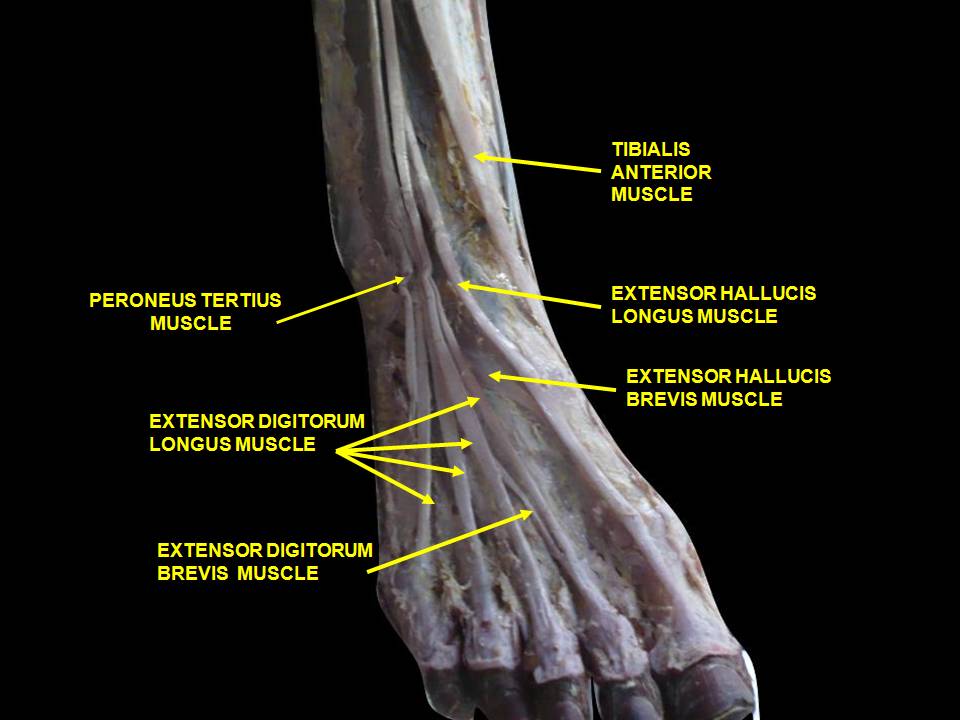
- we have adequate skill, endurance and strength of our extensor hallucis brevis
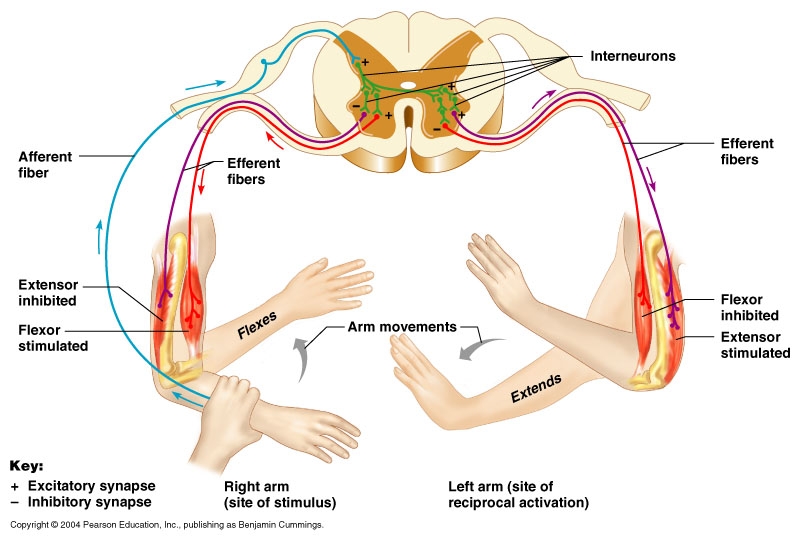
The 1st condition is more global and ensures that our cerebellum and vestibular apparatus are playing nice together to create balance, of the literal sort, We seek to keep our visual axes parallel and our center of gravity over our foot. Remember that the BODY will move itself AROUND the visual axes. If the axes are off, the brain will tilt the head and the body will move AROUND the head to accommodate. We have talked about that in these posts here on the blog.
The 2nd condition, the calcaneo-cuboid locking mechanism, works in the coronal plane and relies on a functioning peroneal group, where the peroneus longus and brevis wrap around the lateral malleolus, cuboid and tail of the 5th metatarsal, crossing the foot diagonally to insert on the base of the 1st metatarsal. When working properly, its actions will be to plantar flex and everting the forefoot, lowering the 1st ray complex down and assisting the shift of the center of gravity more medial for the weight to pass through the medial foot and out through the hallux (ideally).
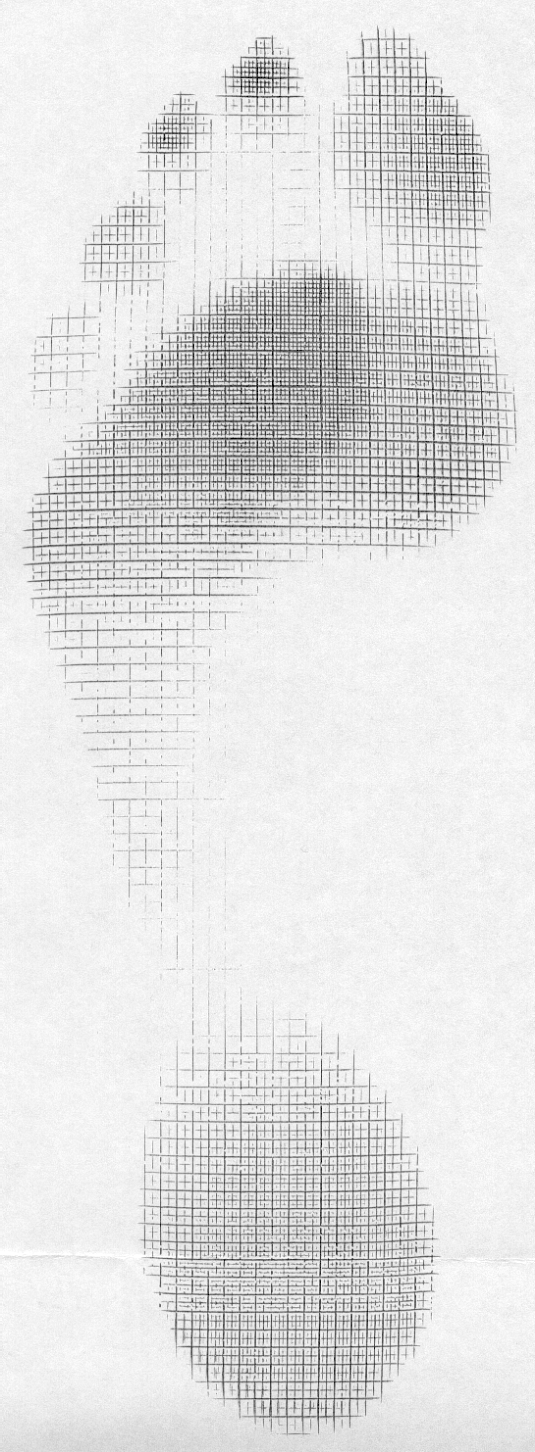
The 3rd condition, the ability to descend the 1st ray, relies on the actions of the peroneus, appropriate supination of the forefoot and ability of the extensor hallucis brevis to do its job. Because the tendon travels behind the axis of rotation of the 1st metatarsal phalangeal joint, in addition to providing extension of the proximal phalynx of the hallux, it can also provide a downward moment on the distal 1st metatarsal (when properly coupled to and temporally sequenced with the flexor hallicus brevis and longus). If the axis of motion for the 1st metatarsal phalangeal joint moves posteriorly, to behind (rather than under) the joint, the plantar pressures increase at MTP’s 4-5 and decrease at the medial mid foot, moving you into low gear push off. If moved even further posteriorly, the plantar pressures, and contact time in the mid foot and hind foot (2). For more on the extensor hallucis brevis, see our post here.
As you can see, high gear is desirable over low gear push off, but sometimes circumstances or biomechanics do not permit. High gear push off ensures the forefoot is dorsiflexed and everted with respect to the rearfoot and the calcaneocuboid and talonavicular joint axes are perpendicular to one another, giving us a rigid lever to push off of as the center of gravity moves medially across the foot. In low gear push off, the foot is inverted and plantarflexed and the stress falls on the lesser metatarsals and lateral stabilizing complex of the ankle, moving the center of gravity laterally, in addition to the calcaneocuboid and subtalar joint axes being more parallel, creating a less rigid lever for push off and decreased mechanical efficiency.
1. Calcaneocuboid joint and stability of the longitudinal arch of the foot at high and low gear push off. J Anat. 1979 Aug; 129(Pt 1): 165–176. link to free full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1233091/
2. van der Zwaard BC1, Vanwanseele B, Holtkamp F, van der Horst HE, Elders PJ, Menz HB Variation in the location of the shoe sole flexion point influences plantar loading patterns during gait. J Foot Ankle Res. 2014 Mar 19;7(1):20.