The case of the dropped (plantarflexed) metatarsal head. Or, “How metatarsalgia can happen”.
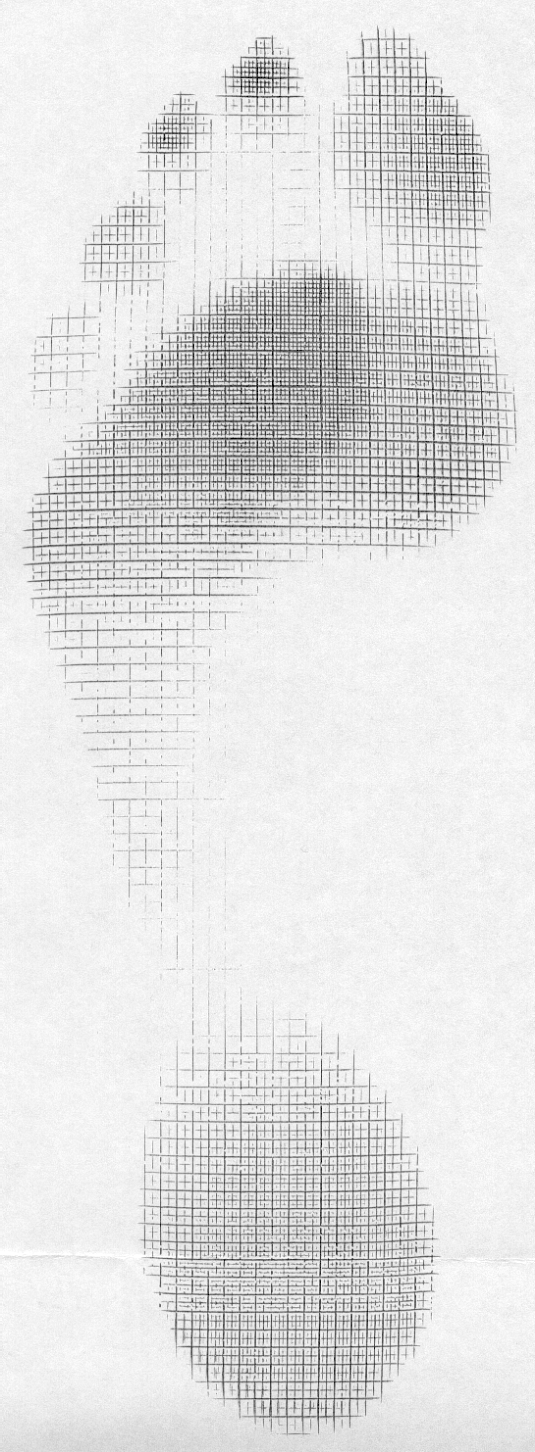
This gentleman came in with fore foot pain (3rd metatarsal head specifically), worse in the AM upon awakening, with first weight bearing that would improve somewhat during the day, but would again get worse at the end of the day and with increased activity. The began insidiously a few months ago (like so many problems do) and is getting progressively worse.
Rest and ice offer mild respite, as does ibuprofen. You can see his foot above. please note the “dropped” 3rd metatarsal head (or as we prefer to more accurately say, “plantarflexed 3rd metatarsal head”) and puffiness and prominence in that area on the plantar surface of the foot.
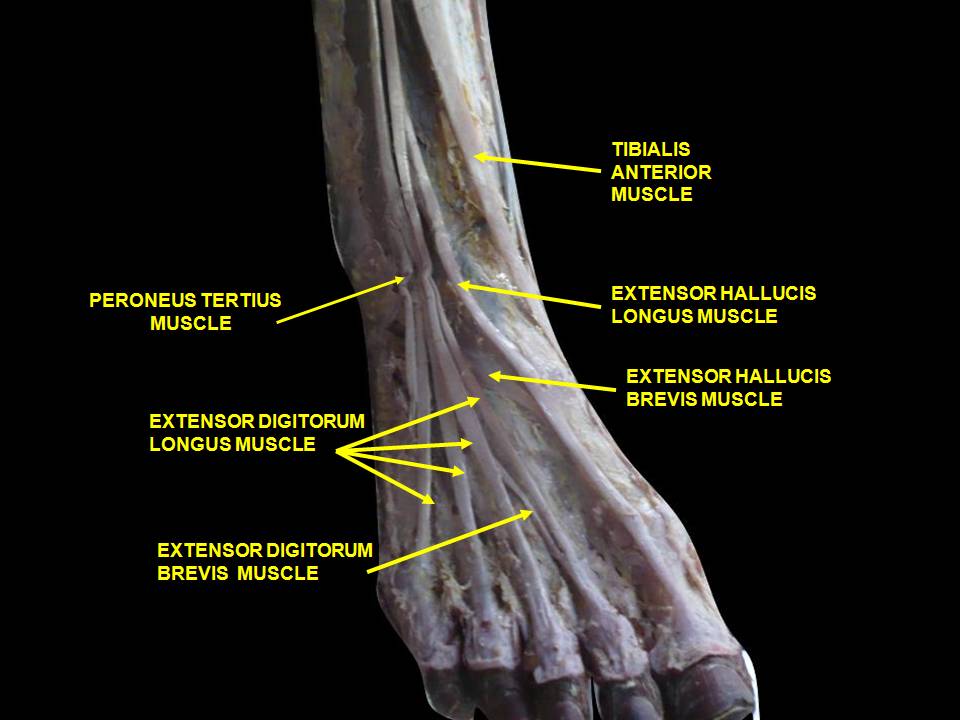
To fully appreciate what is going on, we need to look at the anatomy of the short flexors of the foot.
The flexor digitorum brevis (FDB) is innervated by the medial plantar nerve and arises from the medial aspect of the calcaneal tuberosity, the plantar aponeurosis (ie: plantar fascia) and the areas bewteen the plantar muscles. It travels distally, splitting at the metatarsal phalangeal articulation (this allows the long flexors to travel forward and insert on the distal phalanges); the ends come together to divide yet another time (see detail in picture above, yes, we are aware it is the hand, but the tendon structure in the foot is remarkably similar)) and each of the 2 portions of that tendon insert onto the middle of the middle phalanyx (1)
As a result, in conjunction with the lumbricals, the FDB is a flexor of the metatarsal phalangeal joint, and proximal interphalangeal joint (although this second action is difficult to isolate. try it and you will see what we mean). In addition, it moves the axis of rotation of the metatasal phalangeal joint dorsally, to counter act the function of the long flexors, which, when tight or overactive, have a tendency to drive this articulation anteriorly (much like the function of the extensor hallucis brevis above in the drawing from Dr Michauds book, yes, we are aware this is a picture of the 1st MTP).
Can you see the subtle extension of the metatarsal phalangeal joint and flexion of the proximal interphalangeal joint in the picture?
We know that the FDB contracts faster than the other intrinsic muscles (2), playing a tole in postural stability (3) and that the flexors temporally should contract earlier than the extensors (4), assumedly to move this joint axis posteriorly and allow proper joint centration. When this DOES NOT occur, especially if there is a concomitant loss of ankle rocker, the metatarsal heads are driven into the ground (plantarflexion), causing irritation and pain. Metatarsalgia is born….
So what is the fix? Getting the FDB back on line for one.
- How about the toe waving exercise?
- How about the lift spread reach exercise?
- How about retraining ankle rocker and improving hip extension?
- How about an orthotic with a metatarsal pad in the short term?
- How about some inflammation reducing modalities, like ice and pulsed ultrasound. Maybe some herbal or enzymatic anti inflammatories?
The Gait Guys. Increasing your gait and foot literacy with each and every post.
1. http://en.wikipedia.org/wiki/Flexor_digitorum_brevis_muscle
2. Tosovic D1, Ghebremedhin E, Glen C, Gorelick M, Mark Brown J.The architecture and contraction time of intrinsic foot muscles.J Electromyogr Kinesiol. 2012 Dec;22(6):930-8. doi: 10.1016/j.jelekin.2012.05.002. Epub 2012 Jun 27.
3.Okai LA1, Kohn AF. Quantifying the Contributions of a Flexor Digitorum Brevis Muscle on Postural Stability.Motor Control. 2014 Jul 15. [Epub ahead of print]
4. Zelik KE1, La Scaleia V, Ivanenko YP, Lacquaniti F.Coordination of intrinsic and extrinsic foot muscles during walking.Eur J Appl Physiol. 2014 Nov 25. [Epub ahead of print]