

Iliocapsularis Update
/
As you are probably (hopefully?) aware it has its proximal attachment at the anterior-inferior iliac spine and the anterior hip capsule (1), though it does not attach to the labrum (2). Its inserts distally just south of the lesser trochanter, sometimes inseting into the iliofemoral ligament and/or the trochanteric line of the femur (3,4). It is innervated by a branch of the femoral nerve (L2-4) (4) and is believed to raise the capsule of the hip with hip flexion and be an accessory stabilizer of the hip (1, 2-4, 5)
Since our last article, there has been a few papers published, so here's the update. There has been only one EMG study to date of the iliocapsularis. It found the greatest muscle activity occurred during resisted hip flexion at 90° and lowest activity during hip extension (6). This fits well with its believed function.
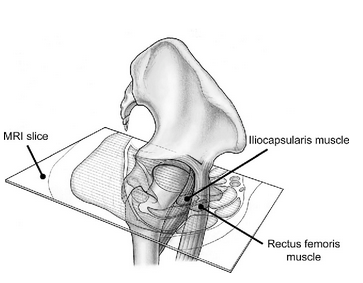
We had discussed previously how it becomes hypertrophied with dysplastic hips (1). A newer study (7) looked at comparing its size in developmentally dysplastic hips vs hips with pincer/CAM type lesions, looking at the iliocapsularis/rectus femoris ratio with it being increased (again) in dysplastic hips.
Finally, 2 new(er) anatomical study (8, 9) confirmed its extensive attachment to the hip capsule, along with the gluteus minimus, reflected head of the rectus femoris, obturator externus and conjoined tendon of the iliopsoas. A bonus of the study revealed the hip capsule was thickest posterosuperior and superolateral on the acetabular side and anterior on the femoral side.
And here is a video on how to needle it...
1. Babst D, Steppacher SD, Ganz R, Siebenrock KA, Tannast M. The iliocapsularis muscle: an important stabilizer in the dysplastic hip. Clin Orthop Relat Res. 2011 Jun;469(6):1728-34. doi: 10.1007/s11999-010-1705-x. Epub 2010 Dec 3.link to full text: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3094621/
2. Anatomy of the iliocapsularis muscle. Relevance to surgery of the hip.Ward WT, Fleisch ID, Ganz R Clin Orthop Relat Res. 2000 May; (374):278-85.
3. HOLLINSHEAD W. H. (ed), Anatomy for surgeons: the back and limbs, vol. 3, Harper & Row, New York, 1969, 707.
4. SUJATHA D’COSTA, LAKSHMI A. RAMANATHAN, SAMPATH MADHYASTHA, S. R. NAYAK, LATHA V. PRABHU, RAJALAKSHMI RAI, VASUDHA V. SARALAYA, PRAKASH An accessory iliacus muscle: a case report Romanian Journal of Morphology and Embryology 2008, 49(3):407–409 link to full text : http://www.rjme.ro/RJME/resources/files/490308407409.pdf
5. Retchford TH1, Crossley KM, Grimaldi A, Kemp JL, Cowan SM Can local muscles augment stability in the hip? A narrative literature review. J Musculoskelet Neuronal Interact. 2013 Mar;13(1):1-12. link to full text: http://www.ismni.org/jmni/pdf/51/01RETCHFORD.pdf
6. Lawrenson P, Grimaldi A, Crossley K, Hodges P, Vicenzino B, Semciw AI. Iliocapsularis: Technical application of fine-wire electromyography, and direction specific action during maximum voluntary isometric contractions. Clin Orthop Relat Res. 2015 Dec;473(12):3725-34. doi: 10.1007/s11999-015-4382-y.
7. Haefeli PC, Steppacher SD, Babst D, Siebenrock KA, Tannast M. An increased iliocapsularis-to-rectus-femoris ratio is suggestive for instability in borderline hips. Clin Anat. 2015 Jul;28(5):665-71. doi: 10.1002/ca.22539. Epub 2015 Apr 14.
8. Walters BL, Cooper JH, Rodriguez JA. New findings in hip capsular anatomy: dimensions of capsular thickness and pericapsular contributions. J Musculoskelet Neuronal Interact. 2013 Mar;13(1):1-12.
9. Cooper HJ, Walters BL, Rodriguez JA1.Anatomy of the hip capsule and pericapsular structures: A cadaveric study. Arthroscopy. 2014 Oct;30(10):1235-45. doi: 10.1016/j.arthro.2014.05.012. Epub 2014 Jul 23.
image credit: Haefeli, Pascal Cyrill et al. “An increased iliocapsularis-to-rectus-femoris ratio is suggestive for instability in borderline hips.” Clinical orthopaedics and related research 473 12 (2015): 3725-34.













