Internal tibial torsion + femoral retrotorsion + twisting = low back pain
/
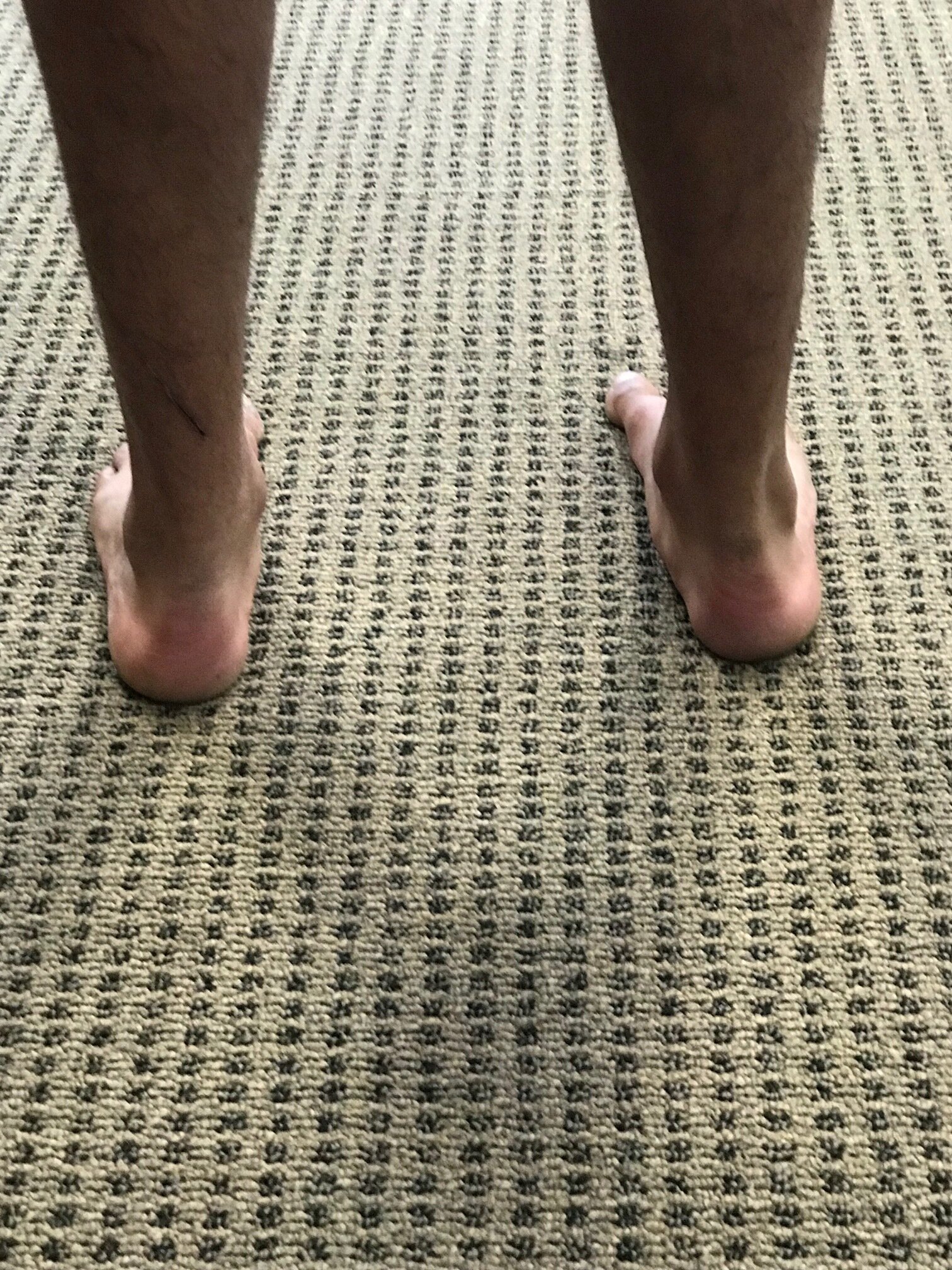
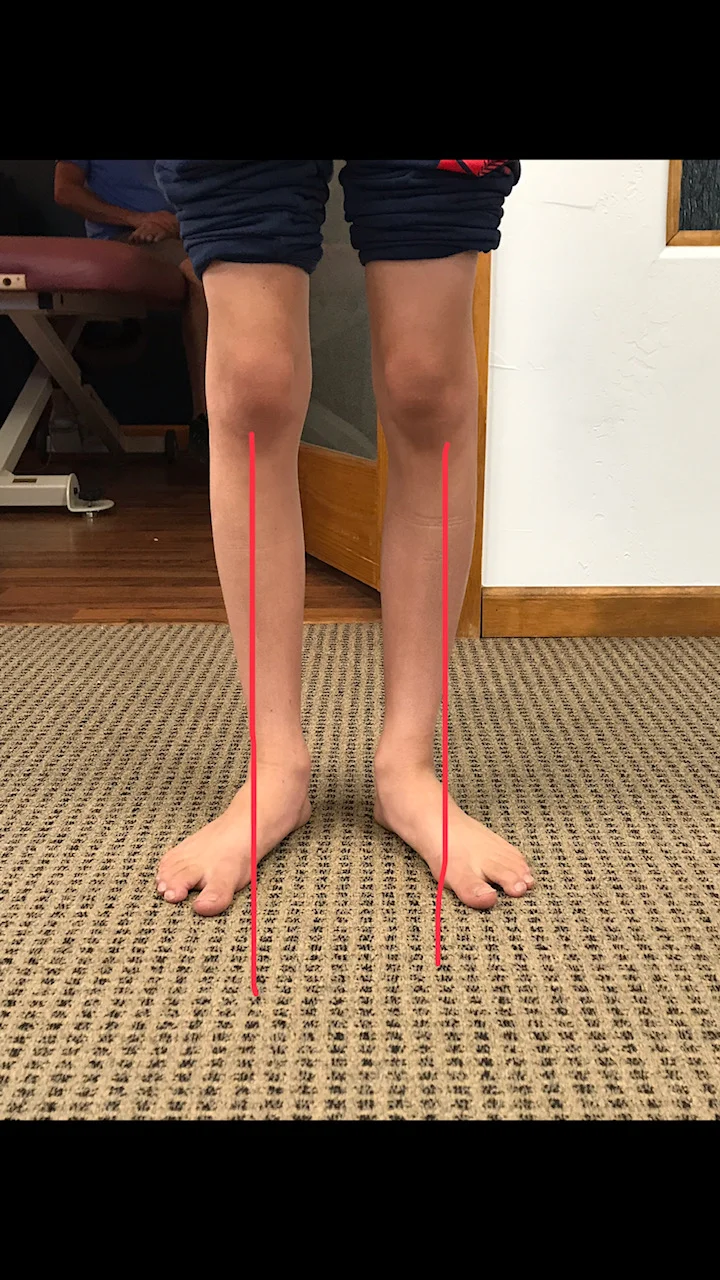
note the internal tibial torsion and lack of internal rotation of the right hip secondary to femoral retroversion

internal rotation of less than 0 on the left hip
Here’s one that we’ve talked about before. Think about internal tibial torsion for a moment. You remember when the tibial tuberosity points straightahead and the foot points inward?
Now combine that with femoral retro torsion. Remember that that’s when the angle of the femoral neck with the shaft is less than 8° which results in a loss of internal rotation of the hip.
Put those two together and you have a foot that points inward and limited internal rotation of the hip on that same side.
Stand on your right leg with your foot turned in. Twist your body to the right. Can you see how this is internal rotation of the right hip?
If people have to create internal rotation of the hip, then the motion has to occur somewhere. If it is not available at the hip and the lower extremity is fully internally rotated it has to occur north of the hip which is usually in the lumbar spine. Now think about when people are lifting things. Often times they do not do a hip hinge and reverse or flatten their lumbar lordosis, opening up the facet joints which allows more rotation. Do you remember that rotation of the lumbar spine is limited to about 5° unilaterally? Where do you think that hip rotation is going to occur? Hmmmm... Probably north of the hip.
Better teach them to spin that weight bearing leg and foot out into some external rotation to create that needed range of motion, increase the amount of internal rotation of that hip or have them keep their shoulders and hips in the same plane when rotating.
Dr Ivo Waerlop, one of The Gait Guys
#backpain #hipinternalrotation #internaltibialtorsion #retrotorsion #femoralretrotorsion