The consequences of an inverted forefoot
/A forefoot that is inverted with respect to the rearfoot. Whether it is a forefoot varus, forefoot supinatus or an everted rearfoot ( because the forefoot is still inverted with respect to the rearfoot), what are the biomechanical sequelae?
If we accept the premise that the foot is basically a tripod between the calcaneus, base of the first and base of the fifth metatarsal‘s, we know that all of these parts needs to be on the ground at certain points in the gait cycle. Forces should travel from the calcaneus, up the lateral aspect of the foot, across the metatarsal heads to the first metatarsal head and hopefully out through the hallux.
The foot should hit the ground in slight inversion of the entire foot at initial contact and pronate through the middle of mid stance and then supinate through the remainder of the gait cycle. There’s an intricate balance of biomechanical events that must occur, especially in the latter half of the gait cycle when the rear foot is inverting where the forefoot is everting, so that we can have high gear push off through the distal first ray.
If the forefoot remains inverted then somehow the head of the first metatarsal needs to be brought down to the ground. If there’s not adequate range of motion in the foot, particularly the first ray, then you may pronate through the midfoot, rearfoot or in cases where this is insufficient, bring them immediately over the foot to get it down. This of course shifts center of gravity to midline and the body above must compensate in someway.
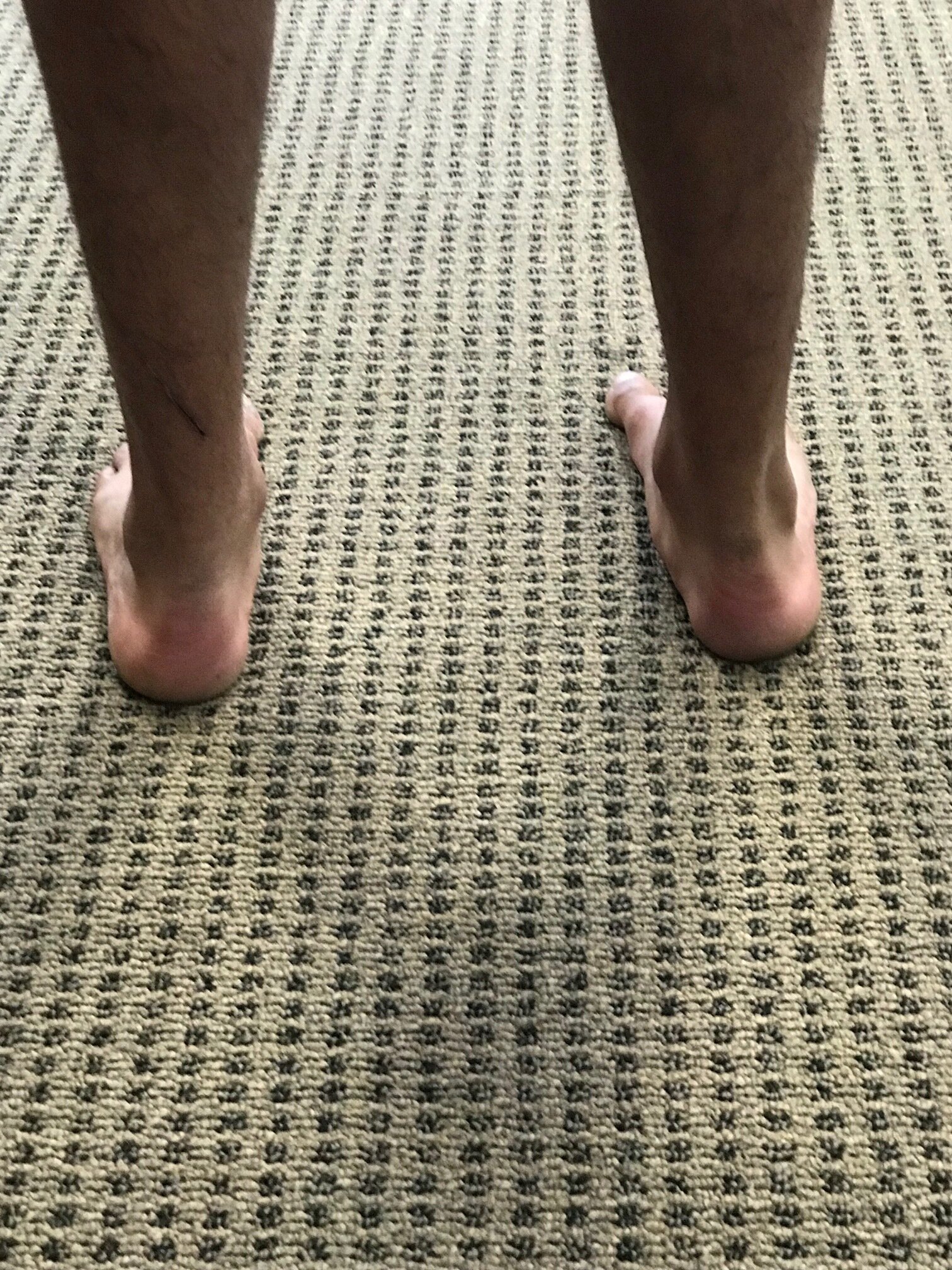
Take a look at this video footage and what do you see? She strikes on the outside of her foot but does not have adequate motion in her forefoot and therefore “crashes“ down on the forefoot, forcing a valgus moment into the ankle and the need to shift immediately by the pelvis attempts to dampen it. Notice how this is worse on the right side with more medial knee shift, pelvic shift as well as a lateral bending of the body to the right. Notice also how the upper body twists more to the left than to the right.
So what’s the fix? Well the answer is, “what’s bothering the patient?” We don’t necessarily fix what we see; we correlate what we see with what the patient’s symptoms are because that’s usually why they show up in your office. Yes, we do get people from time to time that come in strictly for “performance enhancement“ but this is pretty rare.
This woman has very little motion and plantar flexion of the first Ray complex so our primary goal was to get her to descend the first ray. We accomplished this by the following:
1. Manipulation in plantar and dorsiflexion of the first ray complex
2. Soft tissue work in the first intermetatarsal interval
3. Exercises of muscles to assist in descending the first ray including the following: extensor hallucis brevis, peroneus longus, flexor digitorum brevis
4. Pelvic stability work to improve the skill, endurance and strength of the gluteus medius complex as well as abdominal endurance work.
Your rehab program should change as the patient has more functional gains, tailoring it to the patient’s deficiencies.
Dr Ivo Waerlop, one of The Gait Guys
#invertedforefoot #forefootsupinatus #forefootvarus #pronation #forefoot #gaitanalysis