So you want to do a Gait Analysis: Part 4
This is the 4th in a multi part series. If you missed part 1, click here. For part 2, click here, part 3, click here.
These are the basics, folks. We hope this is a review for many.
A quick review of the walking gait cycle components:
There are two phases of gait: stance and swing.
Stance consists of:
- Initial contact
- Loading response
- Midstance
- Terminal stance
- Pre-swing
Swing consists of:
- initial (early) swing
- mid swing
- terminal (late) swing
today, lets explore Terminal stance
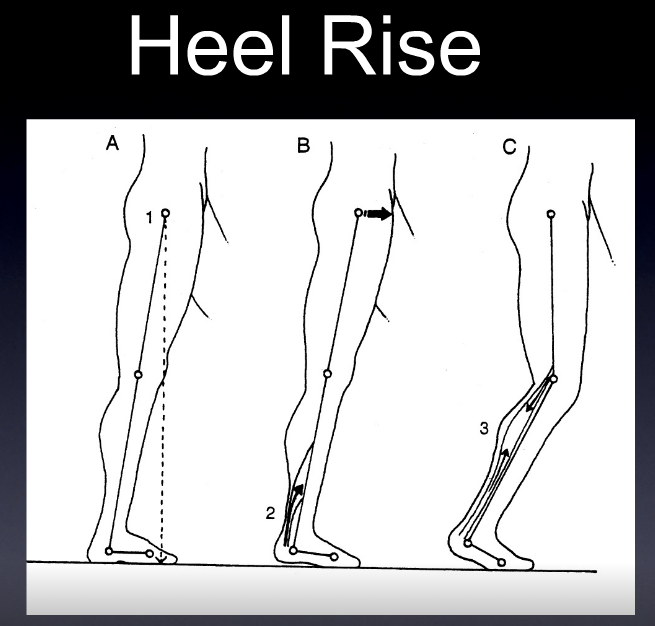
Terminal stance is one of the last stages of stance phase. Following midstance, where maximal pronation should be occurring, the stance phase foot should now begin supinating, initiated by the the opposite foot in swing phase moving forward of the center of gravity.
Lets look at what is happening here at the major anatomical areas:
Foot
- Supination begins from the opposite, swing phase leg (see above)
- the calcaneus inverts to neutral
- the center of gravity of the foot raises from its lowest point at midstance
- The lower leg should begin externally rotating (as it follows the talus)
- The thigh should follow the lower leg and should also be externally rotating; sometimes to a greater extent due to the shape and size of the medial condyle of the femur (which is larger than the lateral)
- these actions are perpetuated by the gluteus maximus and posterior fibers of the gluteus medius, as well as posterior compartment of the lower leg including the flexor digitorum longus, flexor hallucis longus, peroneus longus and tibialis posterior
Ankle
- The ankle should be 5 degrees dorsiflexed and in ankle rocker
- the calcaneocuboid locking mechanism should be engaging to assist the peroneus longus in getting the head of the 1st metatarsal to the ground
Knee
- near or at full extension. This is perpetuated by the quadriceps and biceps femoris, contracting concentrically and attenuated by the semi membranosis and tendonosis. The popliteus contracts eccentrically as soon as the knee passes midstance to keep the rates of external rotation of the tibia and femur in congruence.
Hip
- The hip should be extending to 10 degrees.
Can you picture what is happening? Try and visualize these motions in your mind. Can you understand why you need to know what is going on at each phase to be able to identify problems? If you don’t know what normal looks like, you will have a tougher time figuring out what is abnormal.
Ivo and Shawn. Gait and foot geeks extraordinaire. Helping you to build a better foundation to put all this stuff you are learning on.
pictured used with permission from Foot Orthoses and Other Conservative Forms of Foot Care