The 4 Factors of Heel Rise.
/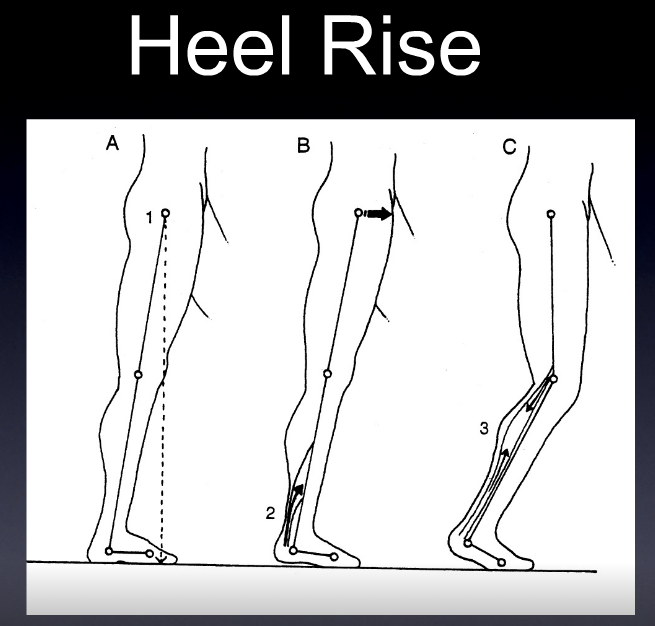

These SHOULD all happen to have appropriate heel rise and forward progression
1. active contraction of the posterior compartment of the calf
2. passive tension in the posterior compartment of the calf
3. knee flexion and anterior translation of the tibia ankle rocker
4. the windlass mechanism
a problem with any one of these (or more collectively) can effect heel rise, usually causing premature heel rise.
ask yourself:
Do you think the posterior compartment is actively contracting? not enough or too much? Remember the medial gastrocnemius adducts the heel at the end of terminal stance to assist in supination. Don't forget about the tibialis posterior as well as the flexor digitorum longs and flexor hallucinate longus.
Does there appear to be increased passive tension in the posterior compartment? How visible and prominent are their calf muscles?
Do they have forward progression of the body mass?
How is his windlass mechanism? Good but not good enough.
Dr Ivo Waerlop. One of The Gait Guys…
#gait, #gaitanalysis, #continuingeducation, #limp, #casestudy, #gaitparameters, #heelrise, #prematureheelrise, #windlassmechanism