Trojan horses for knee menisci.
Orthotics and internal tibial torsion. Good? Bad? or Ugly? It depends…
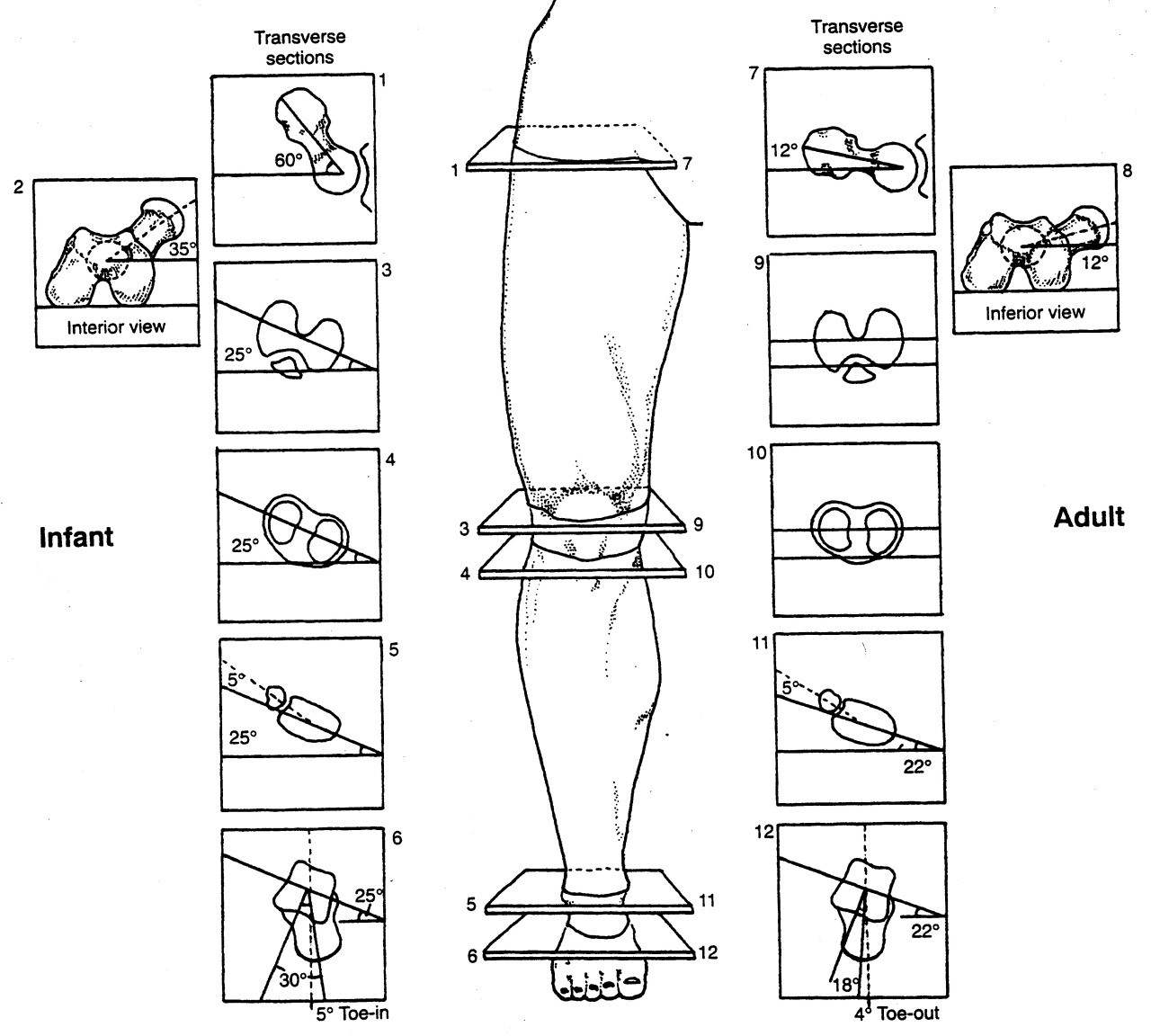
Hopefully you remember about torsions, especially internal tibial torsion (see above). Tibial torsions are deviations (in this case, in the transverse plane) of the long axis of the bone. The bone is basically twisted along its long axis, like wringing out a wet towel. They are measured by drawing an imaginary line through the medial and lateral malleoli, as well as through the two halves of the tibial plateau, and measuring the angle between them (see 2nd picture above). For a more complete review of torsions, click here.
At birth there should be little to no angular difference between the proximal and distal tibia, and this changes to about 19-22 degrees in the adult; the shaft of the tibia rotates outward (externally) with growth resulting in a normal tibial external version (see 3rd picture above). Sometimes, the angular difference is less than zero at birth and the tibia does not rotate outward (externally) resulting in internal tibial torsion.
Internal tibial torsion usually results in a decreased progression angle (more on those here). This often causes a “toed in gait” and the foot remains in supination for a longer period of time (supination is adduction, inversion and plantar flexion), making the foot a rigid lever. When we examine the person in a standing position with the knees in the coronal plane, the feet point inward. When we move the feet to a more normal posture, the knees rotate outward from the coronal plane.
Folks with internal tibial torsion often have a forefoot varus (the forefoot is inverted with respect to the rear foot) because of the amount of supination they are in, which we talked about in the previous paragraph, (see also here). When folks have a forefoot varus, they have a tendency to pronate more through the forefoot, and when people pronate more other folks like to typically put them in orthotics to “get rid of that pronation”(because we all know that pronation is the scourge of humanity, and if there were less pronation in the world, there would probably be fewer wars, famine and poverty : )
So what happens to the knee when we place an orthotic in the shoe? Most orthotics are designed to slow pronation of the midfoot, so they basically supinate the foot, causing the talus to dorsiflex, abduct and invert. This rotates the leg (and thus the knee) externally. With internal tibial torsion, often the knee is already externally rotated because your brain will not allow you to progress forward with your toes in too far, you would trip. So, the orthotic rotates the knee out further, bringing it outside the sagittal plane. This does not bode well long term, as it creates a rotational and friction conflict at the knee (remember the knee is basically a hinge between two ball and socket joints). Guess where the conflict manifests itself? At the meniscus. This, over time, is a great way to macerate a meniscus and create a problem.
Does this mean an orthotic is never indicated? No it does not. It means that if you use one, you should probably make sure the part of the orthotic anterior to the styloid of the 5th metatarsal has a valgus post built into it. This valgus moment will help to bring the knee back to the midline during the propulsive phase of gait. See our recent post here about forefoot valgus posting. Do you think this is ever considered in stores when dispensing foot beds for shoes ? Not all foot beds are evil or a problem mind you, but we have seen some in stores that are real risky business if you ask us.
The bottom line? Know how to use the tools you have available, or someone is going to get hurt. When in doubt, exercise is usually a safer alternative and often has less likelihood of creating a Trojan Horse.
Want to learn more about these kinds of things, foot beds, foot types etc ? Our National Shoe Fit program will help you get smarter about this stuff. email us at : thegaitguys@gmail.com
Gait Guys online /download store:http://store.payloadz.com/results/results.aspx?m=80204
The Gait Guys. Raising questions and providing answers and guidance, with each and every post.
all material copyright 2013 The Gait Guys/ The Homunculus Group. All rights reserved. Please ask before lifting our wares.