

The Knee and Macerating Menisci
/
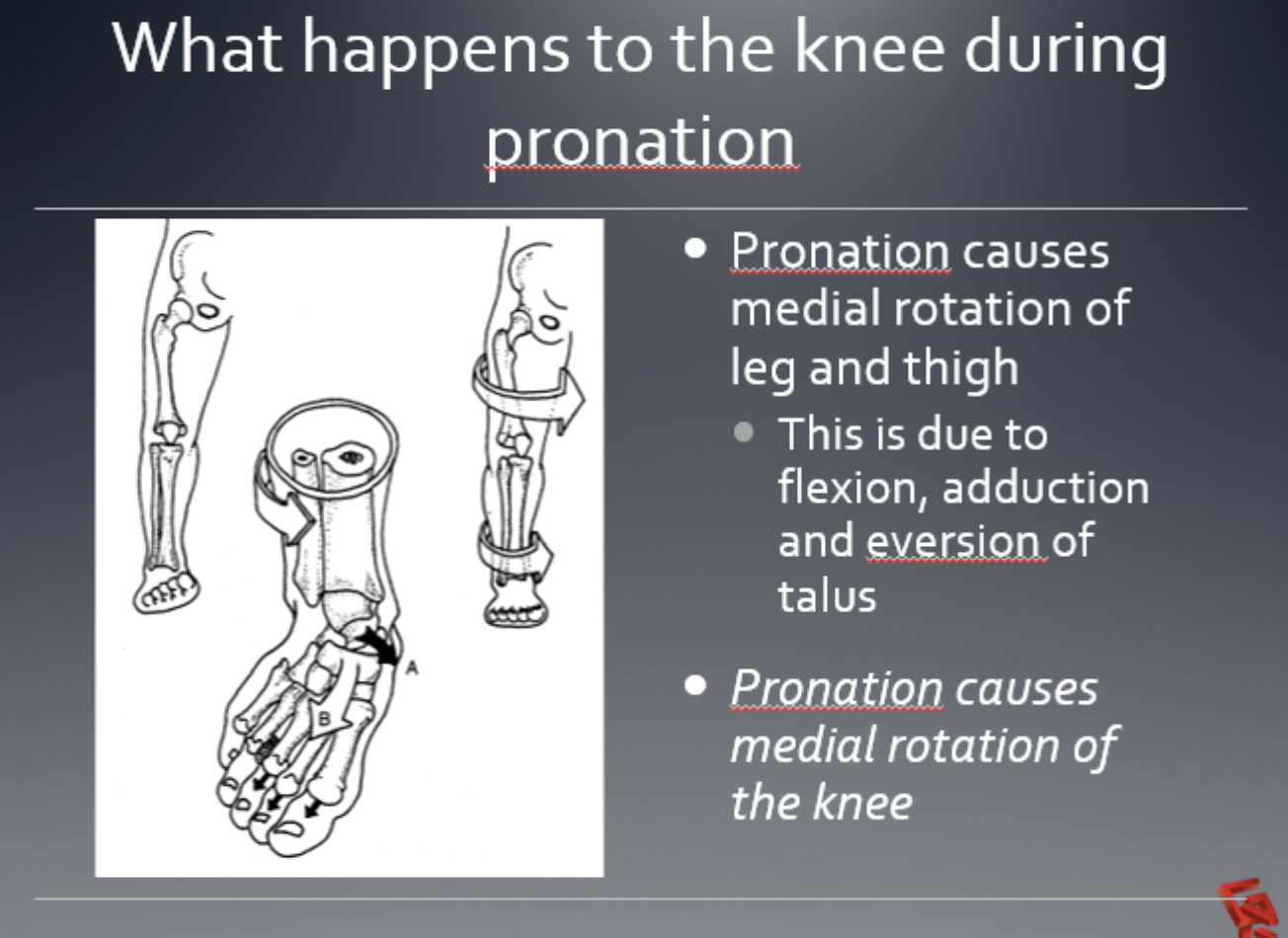
Take a good look at the above 2 slides.
Notice that, during pronation, there is a medial rotation of the lower leg and thigh. We remember that, during pronation, the talus plantar flexes, adducts, and everts. This anterior translation and medial rotation of the talus causes the tibia and subsequently the femur to follow. This, if everything is working right, results in medial rotation of the knee.
From the slides, it should also be evident that the medial condyle of the femur and a medial tibial plateau are larger than the lateral. This allows for an increased amount of internal and external rotation of the knee. We remember that the meniscus, like a washer, is between the tibia and femur. We if you think about this kinematically, it would make sense that the tibia, during pronation (which occurs from initial contact to mid stance) would have to rotate faster than the femur otherwise the meniscus would be caught "in between". If there is a mismatch in timing, the meniscus is "caught in the middle", which causes undue stress and can cause fraying, degeneration, etc.
Likewise, during supination (from mid stance to pre swing) the femur must externally rotate faster then the tibia, otherwise we see this same "mismatch". This is a scenario we commonly see in folks who over pronate at the mid foot and remain in pronation for too omg a period of time.
We think of pronation as being initiated from the movement described above by the talus, and it is attenuated by the popliteus muscle as well as some of the deep flexors of the foot, which fire mostly during stance phase. You will notice that the popliteus is eccentrically contracting at this point.
Supination, initiated by swing phase of the opposite leg and momentum, is assisted by concentric contraction of the popliteus muscle, internal rotation of the pelvis on the stance phase leg, contraction of the vastus medialis, deep flexors of the foot and peroneii.
Taking moment to "wrap your head around" this concept. Now you can see how complicated it can be when we started to throw in femoral and tibial torsions as well as possibly some orthotic therapy. For example, in an individual with internal tibial torsion, if you do not valgus post the forefoot of the orthotic, the knee is placed at outside the sagittal plane in external rotation further by the orthotic and this thwarts the function of his mechanism, leaving the meniscus holding the bag.
Know your anatomy and know what is supposed to be firing when, your patients and clients knees depend on it!


















