More foot exercise studies to confuse you.
/Don't necessarily believe all that you read. Please to not take away from this study that these 4 exercises: short-foot exercise, toes spread out, first-toe extension, second- to fifth-toes extension are golden goose exercises to rehab your athlete. On first glance if one is not thinking, that could be a mistake in translation.
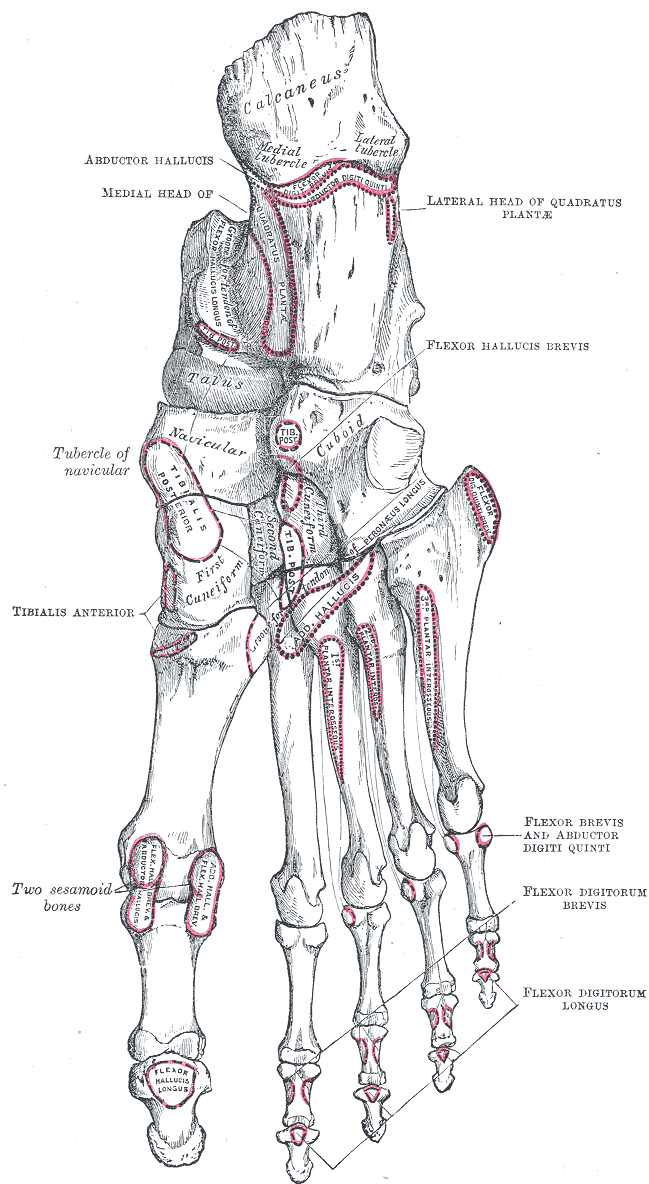
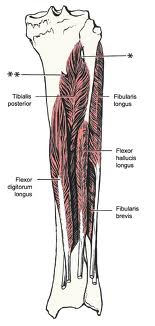
"The intrinsic foot muscles maintain the medial longitudinal arch and aid in force distribution and postural control during gait." That is a pretty bold statement by the study's authors. We would argue that a far less misleading statement would be that "the intrinsic foot muscles are a piece of the puzzle, just a piece, and to dismiss the powerhouse tibialis anterior, tibialis posterior, long and short toe flexors and particularly the extensors is a glaring oversight". Yes, I know, the authors just wanted to study the intrinsics, I get it, -- one just has to be careful of the conclusions made when the study is so microscopic compared to the global perspective at hand. Please, read on.
This study tried to correlate the effects of these 4 exercises: short-foot exercise, toes spread out, first-toe extension, second- to fifth-toes extension on activation of the foot intrinsics muscles they chose to observe (abductor hallucis, flexor digitorum brevis, abductor digiti minimi, quadratus plantae, flexor digiti minimi, adductor hallucis oblique, flexor hallucis brevis, the interossei, and lumbricals).
They looked at the activation before and after exercise in just 8 athletes. They did not look at non-athletes and yes, this is a terribly small N sampling and the study only used T2 weighted MRI to make these conclusions.
The study's conclusion was "Each of the 4 exercises was associated with increased activation in all of the plantar intrinsic foot muscles evaluated.".
Here is my concern*.
Did they consider the various foot typings ? (*Caveat, I have not read the entire study, I am trying to get it). There are many variables to consider including arch integrity, forefoot type, rearfoot type, foot flexibility, step width, step length, client weight amongst other things. Yes, that makes for a near impossible study, I get it. And, it does not appear they had a control study that looked at what happened right after walking. Wouldn't it be fair, and wise, to see what the study showed after barefoot walking for 1-2 minutes ? I bet many of these muscles show significant activation there as well, after all, they were weight bearing and stepping down on the foot which requires the muscles to be activated and utilized. So, does that then mean these 4 exercises are any better than walking ? Does that mean they will suffice for homework for your client ? Does that mean they will strengthen these muscles ? And, does activation mean proper pattern utilization of these muscles, meaning, is there functional translation over to functional use ? Yes, that is not what the study was looking at, but for darn sure that would have been nice info to know. Just take the study for what it found, and do not step beyond those tiny boundaries. We hope that is what they will go for in the next stage of study. To be fair, they also concluded, "These results MAY have clinical implications for the prescription of specific exercises to target individual intrinsic foot muscles." Safe words. Yes, I capitalized the word MAY.
- Dr. Shawn Allen, one of the gait guys.
Thomas M. Gooding, Mark A. Feger, Joseph M. Hart, and Jay Hertel (2016) Intrinsic Foot Muscle Activation During Specific Exercises: A T2 Time Magnetic Resonance Imaging Study. Journal of Athletic Training In-Press.
http://natajournals.com/doi/abs/10.4085/1062-6050-51.10.07
http://dx.doi.org/10.4085/1062-6050-51.10.07