Podcast 151: Gait and neurology of movement, including, Tightness? shortness? What’s the difference? It's the Neurology.
/Truths about Stretching, a case of sesamoiditis, plus exercised induced muscle damage and impaired motor learning, central fatigue, POSE and Chi running and injuries. This is a good one gang, do not miss it !
Links to find the podcast:
Look for us on Apple Podcasts, Google Play, Podbean, PlayerFM, RADIO and more.
Just Google "the gait guys podcast".
Our Websites:
www.thegaitguys.com
Find Exclusive content at: https://www.patreon.com/thegaitguys
doctorallen.co
summitchiroandrehab.com
shawnallen.net
Our website is all you need to remember. Everything you want, need and wish for is right there on the site.
Interested in our stuff ? Want to buy some of our lectures or our National Shoe Fit program? Click here (thegaitguys.com or thegaitguys.tumblr.com) and you will come to our websites. In the tabs, you will find tabs for STORE, SEMINARS, BOOK etc. We also lecture every 3rd Wednesday of the month on onlineCE.com. We have an extensive catalogued library of our courses there, you can take them any time for a nominal fee (~$20).
Our podcast is on iTunes and just about every other podcast harbor site, just google "the gait guys podcast", you will find us.
Where to find us, the podcast Links:
Apple podcasts:
https://itunes.apple.com/us/podcast/the-gait-guys-podcast/id559864138?mt=2
Google Play:
https://play.google.com/music/m/Icdfyphojzy3drj2tsxaxuadiue?t=The_Gait_Guys_Podcast
Other links for today's show:
http://traffic.libsyn.com/thegaitguys/pod_151final.mp3
http://directory.libsyn.com/episode/index/id/11168369
Show notes and links:
We lose muscular Strength as we age.
Changes in supra-spinal activation play a significant role in the age-related changes in strength.
This motor system impairment can be improved by heavy resistance training
https://www.ncbi.nlm.nih.gov/pubmed/25940749
Age (Dordr). 2015 Jun;37(3):9784. doi: 10.1007/s11357-015-9784-y. Epub 2015 May 5.
Strength training-induced responses in older adults: attenuation of descending neural drive with age. Unhjem R1, Lundestad R, Fimland MS, Mosti MP, Wang E.
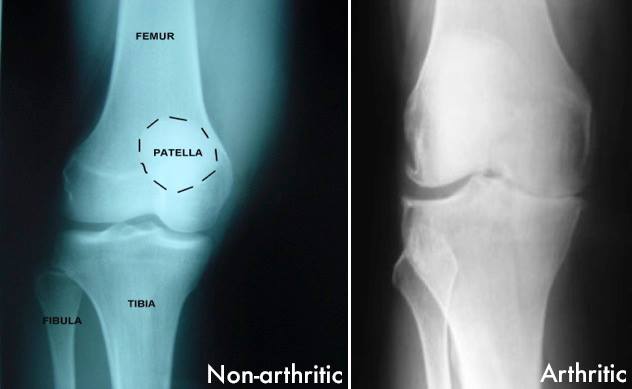
Osteoarthritis and running
https://journals.lww.com/acsm-csmr/Abstract/2019/06000/Running_Dose_and_Risk_of_Developing.5.aspx
Recent literature adds to a growing body of evidence suggesting that lower-dose running may be protective against the development of osteoarthritis, whereas higher-dose running may increase one's risk of developing lower-extremity osteoarthritis. However, running dose remains challenging to define, leading to difficulty in providing firm recommendations to patients regarding the degree of running which may be safe.
Can even experienced orthopaedic surgeons predict who will benefit from surgery when patients present with degenerative meniscal tears? A survey of 194 orthopaedic surgeons who made 3880 predictions
Non-surgical management is appropriate as first-line therapy in middle-aged patients with symptomatic non-obstructive meniscal tears.
https://bjsm.bmj.com/content/early/2019/08/12/bjsports-2019-100567
Sports Biomech. 2019 Jul 31:1-16. doi: 10.1080/14763141.2019.1624812. [Epub ahead of print]
Running biomechanics before and after Pose® method gait retraining in distance runners.
Wei RX1, Au IPH1, Lau FOY1, Zhang JH1, Chan ZYS1, MacPhail AJC1, Mangubat AL1, Pun G1, Cheung RTH1.