You better keep that Hallux Dorsiflexion
/
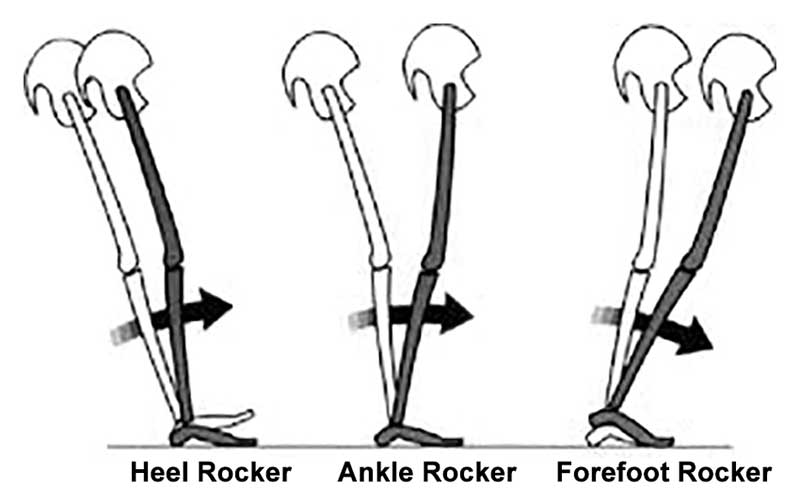
Geee....Looks like forefoot rocker really IS IMPORTANT, eh?
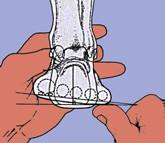
...and what have we been saying about being able to dorsiflex your big toe? Watch how well you or your client can descend the 1st ray (remember that if the head of the 1st does not go down and anchor, its axis of rotation moves dorsally and posterior, limiting dorsiflexion of the joint)
This article should make you look at the "toe break" in a shoe...
"They found that increasing bending stiffness assisted with propulsion during running, reducing the metabolic cost of running by about 1%. However, at a certain level, the increased elasticity began to interfere with the natural flexion of the first MTP joint, reducing the contribution of ankle joint torque to push-off and counteracting the metabolic benefits. Within the study population, the threshold of bending stiffness for optimal energetics varied significantly from one runner to the next, suggesting running shoe design may need to be tuned to an individual runner’s needs."
http://lermagazine.com/news/in-the-moment-sports-medicine/stiffer-shoes-improve-running-energetics-as-long-as-first-mtp-flexion-is-preserved