Why does this gal have so much limited external rotation of her legs?
We have discussed torsions and versions here on the blog many times before. We rarely see femoral antetorsion. She came in to see us with the pain following a total hip replacement on the right.
Note that she has fairly good internal rotation of the hips bilaterally but limited external rotation. This is usually not the case, as most folks lose internal rotation. We need 4 to 6° internal and external rotation to walk normally. This poor gal has very little external rotation available to her.
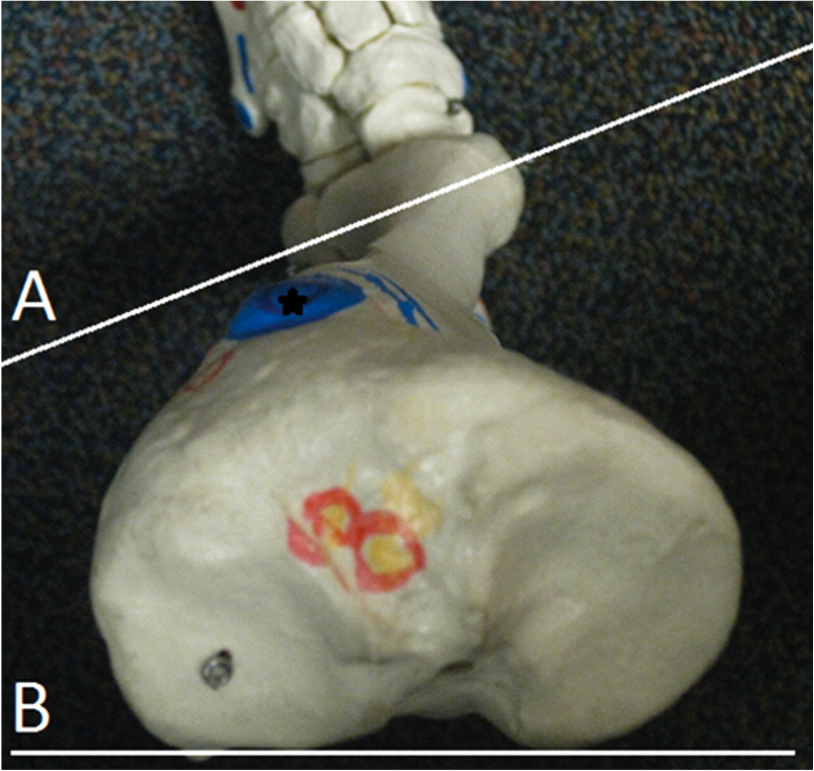
Have you figured out what’s going on with hips yet? She has a condition called femoral ante torsion. This means that the angle of the femoral neck is in excess of 12°. This will allow her to have a lot of internal rotation but very little external rotation. She will need to either “create” or “borrow” her requisite external rotation from somewhere. In this case she decreases her progression of gait (intoed), and borrows the remainder from her lumbar spine.
So what do we do? We attempt to create more external rotation. We are accomplishing this with exercises that emphasize external rotation, acupuncture/needling of the hip capsule and musculature which would promote external rotation (posterior fibers of gluteus medius, gluteus maximus, vastus medialis, biceps femoris). A few degrees can go a very long way as they have in this patient.
confused? Did you miss our awesome post on femoral torsions: click here to learn more.