

We hope you are standing up while you read this….
/
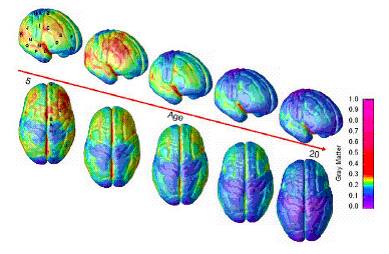
A newborn’s brain is only about one-quarter the size of an adult’s. It grows to about 80 percent of adult size by three years of age and 90 percent by age five (see above). This growth is largely due to changes in individual neurons and their connections, or synapses.
The truth is, most of our brain cells are formed at birth, In fact, we actually have MORE neurons BEFORE we are born. It is the formation of synapses, or connections between neurons, that actually accounts for the size change (see 1st picture above). This is largely shaped by experience and interaction with the environment.
Do you think children’s brains are less active than adults? Think again, your 3 year old’s brain is twice as active as yours! It isn’t until later in life that you actually start dialing back on some of those connections and those pathways degenerate or fade away…a process scientists call “pruning”.
How does this apply to gait? Gait depends on proprioception, or body position awareness. Your brain needs to know where your foot is, what it is standing on and so on. Proprioception, as we have discussed in other posts, is subserved by muscle and joint receptors called mechanoreceptors (muscle spindles, golgi tendon organs and type 1-4 joint mechanoreceptors to be exact). This information is fed to 2 main areas of the brain: the cerebral cortex and the cerebellum. These 2 parts of the central nervous system are interconnected on many levels.
The cerebellum is intimately associated with learning. Try this experiment. you will need a tape recorder (guess we are showing our ages, digital recorder), a timer and a moderately difficult book.
Sit down and pick a section of the book to read. start the recorder and timer and read aloud for 2 minutes. Stop reading, stop the recorder and stop the timer.
Stand up, somewhere you won’t get hurt if you fall. Stand on 1 leg (or if available, stand on a BOSU or rocker board). Open the book to a different spot. Start the timer, the recorder and start reading again for 2 minutes.
Sit back down and grab a snack. Listen to the 2 recordings and pay attention to the way you sound when you were reading, the speed, fluency and flow of words. Now think about recall. Which passage do you remember better?
The brain works best at multitasking and balance and coordination activities intimately affect learning. Having children sit in a class room and remain stationary and listen to a lecture is not the best way to learn. We always tel our students to get up and move around…
This article looks at this relationship in a slightly different way.
The Gait Guys….Sorting it out so you don’t have to.
We hope you are still standing : )
Scand J Med Sci Sports. 2011 Oct;21(5):663-9. doi: 10.1111/j.1600-0838.2009.01027.x. Epub 2010 Mar 11
Motor coordination as predictor of physical activity in childhood.
Lopes VP, Rodrigues LP, Maia JA, Malina RM.
Source
Department of Sports Science, Research Center in Sports Sciences, Health Sciences and Human Development (CIDESD), Bragança, Portugal. vplopes@ipb.pt
Abstract
This study considers relationships among motor coordination (MC), physical fitness (PF) and physical activity (PA) in children followed longitudinally from 6 to 10 years. It is hypothesized that MC is a significant and primary predictor of PA in children. Subjects were 142 girls and 143 boys. Height, weight and skinfolds; PA (Godin-Shephard questionnaire); MC (Körperkoordination Test für Kinder); and PF (five fitness items) were measured. Hierarchical linear modeling with MC and PF as predictors of PA was used. The retained model indicated that PA at baseline differed significantly between boys (48.3 MET/week) and girls (40.0 MET/week). The interaction of MC and 1 mile run/walk had a positive influence on level of PA. The general trend for a decrease in PA level across years was attenuated or amplified depending on initial level of MC. The estimated rate of decline in PA was negligible for children with higher levels of MC at 6 years, but was augmented by 2.58 and 2.47 units each year, respectively, for children with low and average levels of initial MC. In conclusion MC is an important predictor of PA in children 6-10 years of age.
© 2009 John Wiley & Sons A/S.





















