The Banana Toe: The Force has to go somewhere. It’s a Jedi Gait Rule.
* note: there are 4 photos to today’s blog post. Be sure you click through all 4.
When you toe off, you have to toe off from somewhere in the foot unless you like an apropulsive hip flexion gait, where you just lift you foot off the ground from foot flat, kind of like a true neurologic “foot drop” gait client would. But, if you are lucky enough not to have a true foot drop, you are going to push off somewhere in the foot. You can do it off the lateral foot (low gear toe off) and lesser toes, or you can do it off the big toe (high gear) the way we were built to do it.
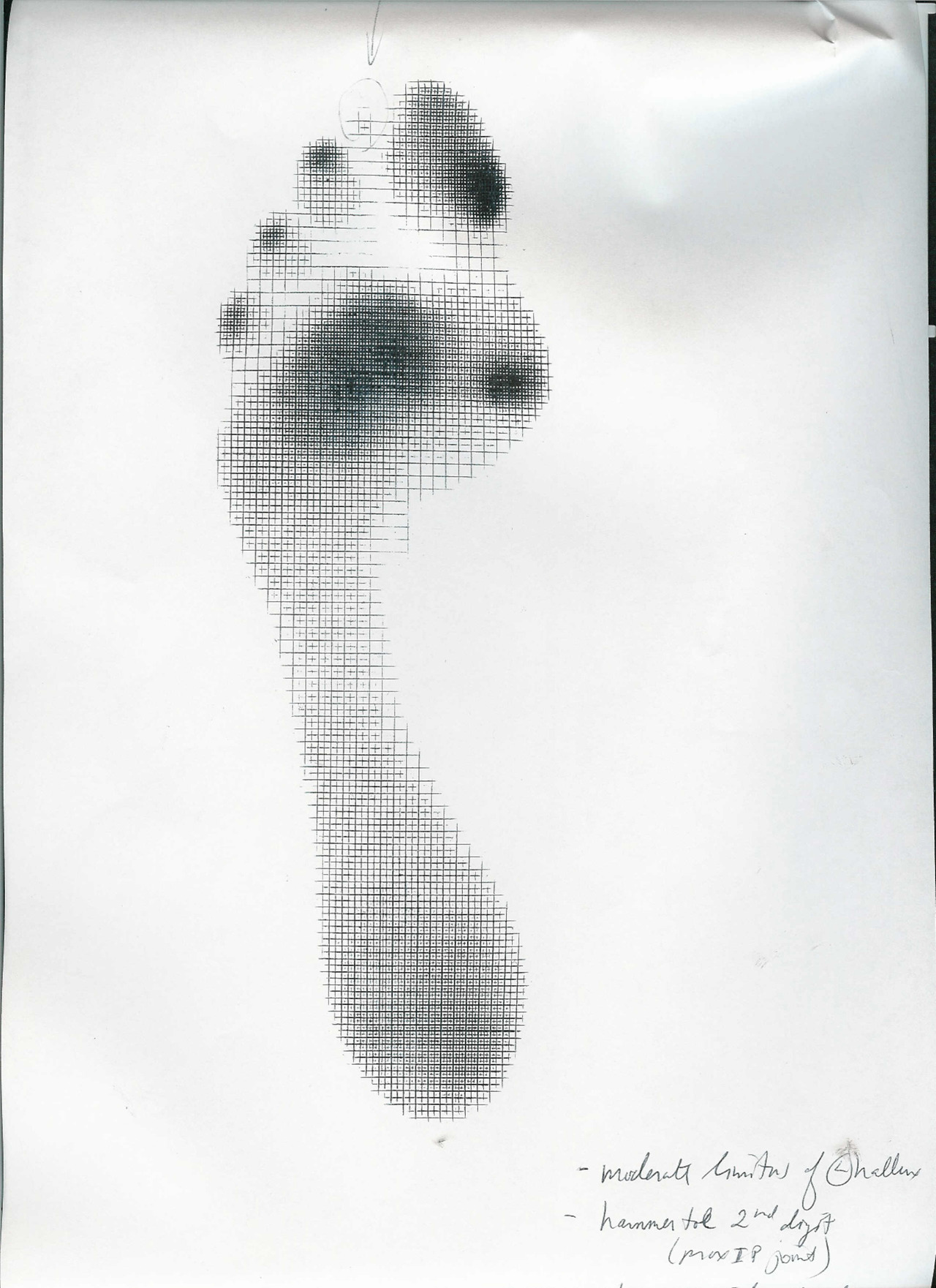
The above pictures show a nasty dorsal crown of osteophytes that is limiting hallux (big toe) extension/dorsiflexion. This is true hallus rigidus and hallux limitus. When this client attempts to toe off, the joint cannot normally partake in the activity, there is no Windlass effect, no posturing up over the sesamoids for mechanical advantage etc.
In this scenario, there are two places you can put it, up into the next proximal joint(s) meaning the met-cuneiform joint or further down into the interphalangeal joint. In other words. the loads go proximal or distal to the limited joint, and they eventually play out there, over and over and over gain. The former option would basically mean you are pronating/dorsiflexing through the midfoot which is never good (can you say Saddle exostosis ! ouch !) or the latter option is to dorsiflex through the interphalangeal joint and over time that toe begins to attenuate plantar ligamentous structures and extend beyond its normal limits resulting in the “Chiquita” toe (a upward bent toe resembling a banana shape). This will disable the long flexor of the great toe (FHL: flexor hallucis longus).and inhibit mechanical advantage of the extensor digitorum brevis. If you struggle with the “how and why” behind this sentence in terms of restoration attempts, you need to watch my video here. It will offer you deeper insights.
Will this toe become painful ? yes, in time it is quite possible. Is there much you can do? Sure, a rocker bottomed shoe will help take the load at toe off instead of forcing it into this toe or the midfoot. Will an orthotic help ? Well, this is a loaded question. If you are putting the forces into the midfoot choice as described above, the orthotic will block that motion and you will likely default option into the toe presentation above. So you are merely just moving loading forces around. It can be helpful, but you are quite possibly “robbing Peter to pay Paul” as they say. The video I asked you to watch can be helpful but it will force that metatarsophalangeal joint into extension, a range it does not have, so it is not a remedy and not recommended. Perhaps some awareness and slight increase in FHL(long toe flexor) use can be attained however. These are tricky cases, simple in theory, but execution can be fussy and requires patient awareness and education. We like the rocker bottomed shoe as a nice easy solution and some increased FHL use awareness. Help them find a little more FHL use by putting a pencil under the crease of the toe and help them to drive the tip of the toe down just a little out of that banana extension posture. It can help them control the overloading of the dorsal aspect of the interphalangeal joint.
As always, lets carry this forward into gait thoughts. How is hip extension going to be in this client ? How is glute strength ? Hip joint range ? Hip extension motor patterning ? Will the client go into anterior pelvic tilt to borrow the last range of hip extension ? Will the hamstrings have to accommodate ? Lots of yummy biomechanical and neurological mental gymnastics here. Bottom line answer to all the above ? “ it depends, they will have to accommodate and compensate”. And as the Jedi Gait Rule goes, “the Force as to go somewhere”.
Shawn Allen, one of the gait guys