Vintage Nike Niobe
I best recall being told that this shoe was worn three times, the third run was a marathon, and as you can see that was its last day on the road.
This is what happens when someone who should not be in a curve lasted shoe, chooses to run in one. The Nike Niobe was a curve lasted simple shoe. It was very light weight, small stack height and narrow ramp from heel to forefoot. This was likely a fast shoe for someone, for the right foot type.
This person was obviously having some distal toe pain, so they pre-shredded the tip of the shoe to offer some “space”. Perhaps they were sized wrong, perhaps this person had a tender 2nd toe/nail. But this is not the purpose of today’s blog post.
Today we wanted to bring up shoe LASTS again.
The Last (the part between the midsole and insole)
Strictly speaking, a last is the mold or template for creating the shoe. It defines theshape of a shoe. Remember that men’s and women’s feet are shaped differently. Men (usually) have rectangular feet (the forefoot and heels are wider, or have less difference in width); Ladies (usually) have triangular feet (the forefoot is much wider than the heel). This is why it is important to know if the shoes you are fitting are a men’s or women’s specific last. Many times, the shoes come off the production line and the boy shoes are blue and the girls pink: both made from the same last.
The last determines whether a shoe is a high, medium or low volume shoe… Pretty important, if they have a high instep or flat foot. Companies like Altra have as many as 6 different, sex specific lasts. This results in a wide range of fit (and thus a bigger market share).
Take off your clients shoes and look at their feet. Note their shape and curve. Lasts need to match that “curve” so they can be relatively straight or curved (this refers to the shape of the “sole” of the shoe: see above). Turn a shoe over and look at the sole. Mentally bisect the heel with a line going to the front of the shoe. If the line bisects the front of the shoe, it is a straight lasted shoe (this corresponds to the axis of the 2nd metatarsal, or slightly lateral to it). If more of the shoe falls medial to this (more of the sole on the big toe side) it has a curved last.
Curved last shoes can vary in the degree of curvature. Curved last shoes are designed to help control pronation, as they provide medial support and slow its rate by causing a relative supination of the foot after heel strike (it weights the lateral border of the shoe for a longer period of time, theoretically allowing less pronation). Curved last shoes can put more motion into a foot, especially one with limited rearfoot motion (it still must pronate, but due to the lack of rearfoot motion, the forefoot must compensate and now must do so in a shorter period of time).The last is the surface that the insole of the shoe lays on, where the sole and upper are attached. Shoes are board lasted, slip lasted or combination lasted. A board lasted shoe is very stiff and has a piece of cardboard or fiber overlying the shank and sole (sometimes the shank is incorporated into the midsole or last) . It is very effective for motion control (pronation) but can be uncomfortable for somebody who does not have this problem. A slip lasted shoe is made like a slipper and is sewn up the middle. It allows great amounts of flexibility, which is better for people with more rigid feet. A combination lasted shoe has a board lasted heel and slip lasted front portion, giving you the best of both worlds.
When evaluating a shoe, you want to look at the shape of the last (or sole). Bisecting the heel and drawing an imaginary line along the sole of the shoe determines the last shape. This line should pass between the second and third metatarsal. If you do this to the Nike Niobe shoe you will see a nice gentle curved line, it is not as much as one would think because the severity of the carved away instep/arch gives it the appearance of a more curved last than it truly is. Drawing this imaginary line, you are looking for equal amounts of shoe to be on either side of this line. Shoes have either a straight or curved last. The original idea of a curved last (banana shaped shoe) was to help with pronation. A curved last puts more motion into the foot and may force the foot through mechanics that is not accustomed to. Most people should have a straight last shoe. Folks who have pronation challenges will do better with a semi-curved to straight lasted shoe. Few people need a truly curve lasted shoe. A general rule of thumb is: You really can’t go wrong with a straight last. It will work for all feet, especially if you are using an orthotic. This is especially important with people with forefoot abductus, moderate to severe pronators and rigid feet (rear or forefoot). A forefoot abductus and severe pronator’s feet will move laterally in the shoe, often causing crushing, rubbing, cramping and blistering of the little toe against the side of the shoe. A rigid foot, because the foot needs to be able to pronate at the mid and forefoot, will have a similar problem. You can use a curved last with people with mobile or hypermobile feet, provided their pronation is not too severe (clinical judgment, trial and error).
You won’t see any Nike Niobe’s anymore, they are even mere ghost stories even on the internet. It is cool to see where shoe fabrication logic was long ago, and to see how far it has come. RIP Niobe.
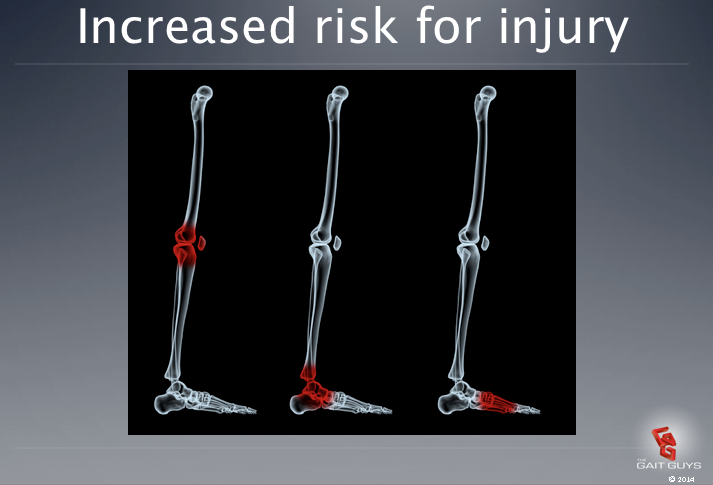
This was clearly an example of a heavy pronator (note the medial heel blow out) starting at the rearfoot heel contact. They were also likely a heel striker, but that was “the thing” back then. The gentle curve in this shoe’s last did not do this person any favors, heck this runner was likely crippled for a week with arch pain, tibialis posterior pain and medial knee pain. A shoe can really tell a story !
Want to learn more about shoe anatomy and how to pair shoes to certain foot types ? Do you find yourself wanting to know more about a forefoot varus, forefoot valgus, compensated and uncompensated variants of these or rearfoot variances ? Here is where you should start:
Gait Guys online /download store (National Shoe Fit Certification and more) :
http://store.payloadz.com/results/results.aspx?m=80204
Or, other web based Gait Guys lectures: www.onlinece.com type in Dr. Waerlop or Dr. Allen, ”Biomechanics”
Thanks to Wayne over at Dick Pond Shoes for this little gift 10 years ago. We came across it doing some thinning out of “the herd” of great shoe pathology samples we like to keep.
Shawn and Ivo, The Gait Guys