Short leg and Pronation
/Dr Allen was ON FIRE on tonites onlinece.com lecture Biomechanics 322). Hope you will join us again (or next time if you missed us). We talked about many of the aspects of a static exam and how it effects weight bearing in the foot. The word "short leg" came up more than once, and yes, from Dr Allen : )
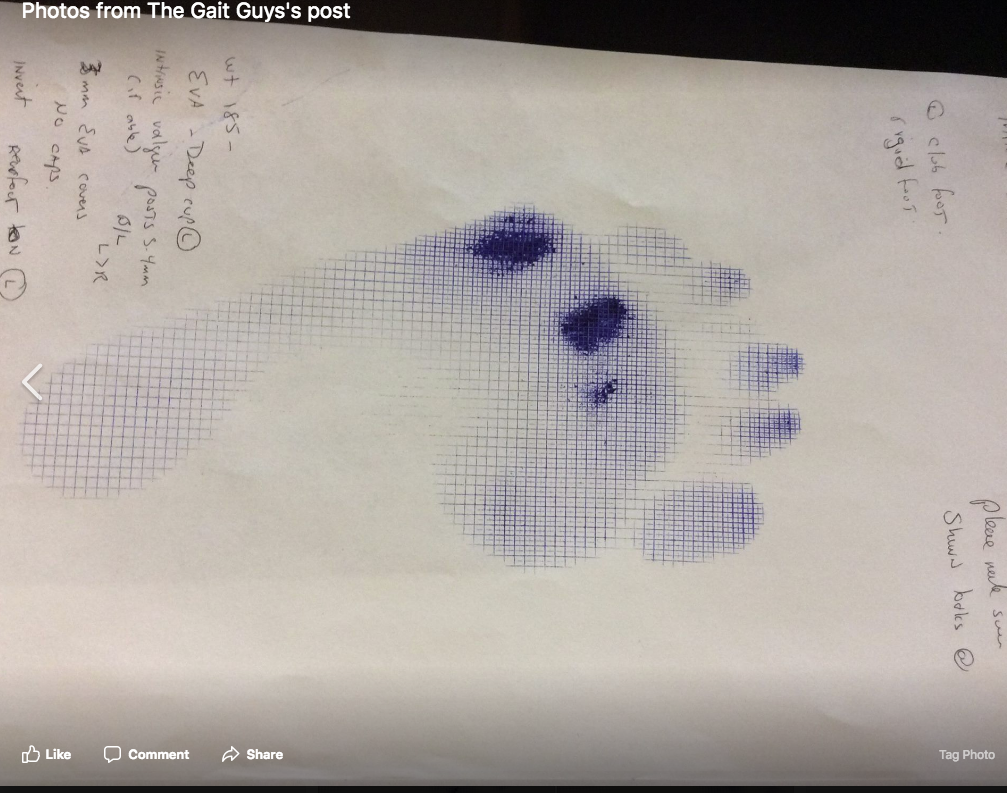
Remember, as the foot pronates more on one side, the center of gravity will move medially. You will often see more toe clenching (and resultant quadratus plantae weakness) on the more pronatory side and more toe elongation on the more supinatory side. You will often also see more splay and elongation on the pronatory side, and less elongation and less splay on the supinatory side. Remember, these are guidelines and not rules, and there are ALWAYS exceptions.