The Black Plague (ok, kinda sort of)……Subungal Hematomas in Runners. Blood under the toe nail. Not what you think it is from !
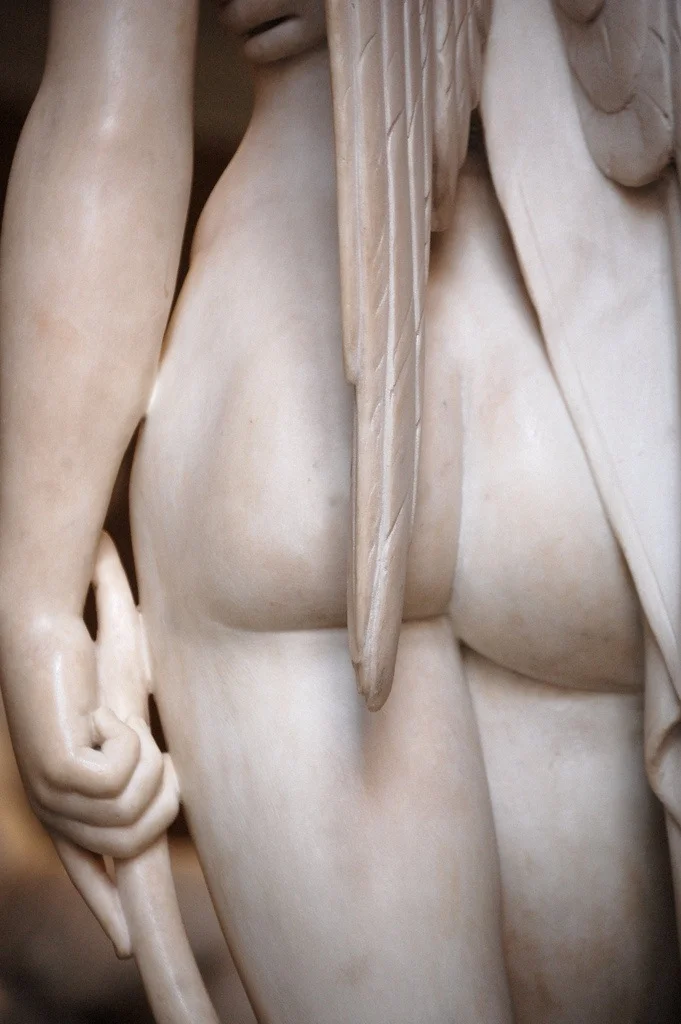
There are two pictures here, cursor to the right and see the slider that will toggle between the two photos. The photo with bandaid credit given to www.healthandrunning.com the other photo……is a runner client of ours with both a callus pattern on the tip of the 2nd toe and an early small subungal hematoma (read on !)
__________________________________________________________________________
We get inquiries about the black toe nail “Syndrome”……aka…..blood under the toe nails in our runners, and how to avoid them. Lets look at this phenomenon as it pertains to the foot.
This problem has a clinical name, “subungual hematoma”. It means a collection of blood under the finger or toe nail. There are many causes of the subungal hematoma (SH for short as we move forward here). Here are a few, but we have yet to find any good journal articles for one cause that we are seeing as a possible cause…one we will discuss here shortly.
One cause is obvious, the crush injury where someone steps on your toe, you drop something onto it or smash it into something. This is something we have all done at some time.
The most commonly theory of cause is repetitive trauma, thought to be that of repeated impact of the toe into the top or end of the shoe. Heim et al noted this in 2000. This really got us to thinking. Why, when we see these SH’s, do the runners never seem to have shoes that are too short / small or shoe signs of friction (wear patterning) of the toe nail into the top of the shoe’s upper ? Often the runners insist there has been no such contact within the shoe. So we started our own investigation making sure to ask all our runners what they thought and felt as they ramped up their miles in prep for marathons and 20 mile runs or daily doubles, particularly those who seemed regularly susceptible to SH’s. We will discuss our findings and thoughts momentarily, but lets get back to some of the more well known information on SH’s.
The medical literature is full of other types of causes or clues of SH’s that must be investigated, such as medication reactions, autoimmune skin disorders, melanoma, blood disorders (dyscracias or clotting problems). These certainly are not the norm.
It is important to know the anatomy of the area because the nail bed is very rich in vasculature (hence the hematoma creation) and nerve endings (hence the pain) when blood collects in the confined area or it gets torn off from trauma. The nail bed is a derivative of the epidermis containing keratin which gives it its hard nature. The nail grows from a nail root in front of the cuticle and grows distally at a slow but (usually) steady rate. This area is frequently susceptible to fungal infections which destroy the tissue in the area and possibly make SH’s more common.
We will not get into the aggressive treatment of things here because that is 1) not our purpose here and 2) we do not want to be accountable for people getting infections from boring a hole into the nail bed (trephine) to release the blood or the consequences of using plyers to yank it off. We just tend to recommend they be left alone and let nature take its course. (For those bold and tough gang, who chose the plyers method, you should know that there is no fatty tissue beneath the nail and the underlying bone to cushion the area, the nail is the only protection; furthermore you should know that the extensor tendon attachment is awfully close to the proximal nail bed root area !). But when pain it too much, we have our people we refer these cases to. Rather, we tend to look for a cause of the problem.
In a limited number of cases we do see a shallow toe box where there is little room for toe extension, thus the nail can get rubbed on the roof of the toe box repeatedly causing a lifting action of the nail from its vascular bed. This a more plausable cause in our opinion over the “toes hitting the end of the shoe” phenomenon put out there by many sources. Particularly when most people size their shoes sufficiently long enough for the distal foot slip migration that occurs at mid-foot load within the shoe. In these cases a close cropping of the toe nail shoe stop the lifting/friction phenomena on the toe box roof.
However, we seem to be seeing a more frequent trend that we wanted to share here. It seems to go hand in hand with the plague of flexor dominance in our society these days. What we are seeing is a predominance of toe flexion (either a gentle or marked toe flexion ….we sometimes refer to it as toe hammering) in our runners. This just makes sense because of the posterior compartment dominance in runners. (The posterior compartment is made up of the gastroc-soleus complex, long toe flexors and tibialis posterior). So if this compartment is dominant, and there is not sufficient home work to off set the flexor dominance with extensor exercises, then this flexion dominance will continue and possibly worsen. As you will see either in yourself, our photo here, or on the feet of many of your co-runners is a distal “tip of the toe” callus development (usually most on the second toe, and less moving into the more lateral toes) immediately below the leading edge of the toe nail. This callus coincides well with a distal gripping phenomenon of the long flexors (Flexor digitorum longus). So, now imagine, to get the callus there must be repeated friction and since the toe is not hitting the end of the shoe it must be friction into the sock liner bed of the shoe. And if this is the case, the skin is pulled at a differential rate over the distal phalange than the nail bed there will be a net lifting response of the nail from its bed as the skin is drawn forward of the backward drawn phalange (put another way, the callused toe tip is fixed to the sock liner for grip, and then the phalange is drawn backwards from this contact point creating a NET movement of skin forward thus lifting the nail from its bedding). [For an at-home example of this, put your hand flat on a table top. Now activate your distal long finger flexors so that only the tip of the fingers are in contact with the table top. Now, without letting the finger tip-skin contact point move at all, go ahead and increase your long flexor tone/pull fairly aggressively. I defy you to not feel some pressure building under the distal tip of the finger nail as the skin is RELATIVELY drawn forward.] And with the nail bed being so vascular, micro bleeding can occur. This bleeding is slow and takes time. Which brings the big question to light, SH’s seem to mostly occur on very long runs, and never on short runs (where there is not enough nail bed separation repeatedly to create enough damage to bleed, not to mention fatigue of the other toe/foot intrinsic muscles thus necessitating more use of the more powerful long toe flexors.)
There does not seem to be anything out there in the information on this supposition. Maybe we are crazy…….but we do see alot of runners. And once we bring the awareness of the problem to our runners and show them how to reduce the flexion dominance with exercises to gain more extension balance, do we see an arrest of any further Subungal hematomas.
We would love to hear your thoughts and experiences with them, both clinically and as a runner. Let us know what you think about our plausable cause.
we remain……The Gait Guys